
RESEARCH ARTICLE | DOI: https://doi.org/dx.doi.org/JMMRCT/PP.0002
Oral and maxillofacial surgeon,Anandaban Hospital, Position 11th level. Head of the department, Nepal.
*Corresponding Author: Bikash Desar
Citation: Bikash Desar, (2026) Oral Manifestations in Patients with Leprosy Visiting Anandaban Tertiary Hospital and Their Impact on Patients’ Quality of Life, J. Modern Medical Research and Clinical Techniques1(1): dx.doi.org/JMMRCT/PP.0002
Copyright  :
© 2026 Bikash Desar. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
:
© 2026 Bikash Desar. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 January 2026 | Accepted: 28 February 2026 | Published: 23 March 2026
Keywords: tongue, lips, hard palate, buccal mucosa, uvula, faucial pillars and gingiva
Background: Leprosyis a chronic infectious disease caused by Mycobacterium leprae, primarily affecting the skin and peripheral nerves. However, several otherorgans and tissues may also be involved, including the liver, kidneys, eyes, lymph nodes, bones and joints, gonads, and theoral cavity. Oral manifestations of leprosy can involve variousstructures such as the tongue,lips, hard palate,buccal mucosa, uvula, faucial pillars, and gingiva.
Aim:The aim of this comprehensive reviewis to raise awareness among dental professionals regarding the classification, pathogenesis, clinical features, diagnosis, management, leprosy reactions, and oral manifestations of leprosy. Increased awareness among dental professionals can contribute to the earlydetection, timely referral, and effective management of patients with leprosy.
Methods:A comprehensive electronic literature search was conducted using Google Scholar and PubMed to obtain relevant data on the classification, pathogenesis, clinical features, and oral manifestations of leprosy.
Results:A totalof 14 articles were selectedand reviewed to analyze the classification, pathogenesis, clinical features, and oral aspectsof leprosy.
Conclusion:A thorough oral examination may contribute significantly to the early diagnosis and prompt management of leprosy. Enhanced awareness and involvement of dental professionals in recognizing oral manifestations can improve timely referral and overall patient outcomes.
Leprosy, also known as Hansen’s disease, is a chronic infectious condition. The averageincubation period ranges from approximately 3 to 10 years. The infection is primarily transmitted through prolonged and close contact with individuals affected by leprosy. Clinically, leprosy presents in two polar forms: tuberculoid leprosyand lepromatous leprosy, both of which are immunologically stable. In contrast, the borderline and indeterminate forms are considered immunologically unstable. The Ridley– Jopling classification, proposed in 1966, categorizes leprosy into different forms based on clinical features, histopathological findings, and the host’s immune response.
Another classification of leprosy is based on the number of skin lesions and bacillary load, categorizing the disease into paucibacillary and multibacillary forms. Paucibacillary leprosy, which includes tuberculoid leprosy, is characterized by the presence of five or fewer skin lesions and may involve sensory loss due to involvement of a single peripheral nerve trunk [3,4]. In contrast, multibacillary leprosy, which includes lepromatous leprosy, presents with more than five skin lesions and may involve sensoryloss due to the involvement of two or more peripheral nerve trunks [4].
This review article addresses the classification, pathogenesis, clinical features, diagnosis and management, leprosyreactions, and the oral aspects of leprosy. Oral manifestations are most commonly associated with lepromatous leprosy. Increased awareness among dental professionals regarding the various aspects of leprosy can contribute to improveddiagnosis, referral, and treatment planning for affected patients. This review emphasizes enhancing the understanding of oral manifestations of leprosy among dental professionals, highlighting the importance of thorough oral examination and appropriate referral to dermatologists for comprehensive evaluation of other systemicinvolvement.
Comprehensive data were obtained through an electronic literature search of Google Scholar and PubMed focusing on the classification, pathogenesis, clinical features, diagnosis and management, leprosy reactions, and oral manifestations of leprosy. Studies published between January 1, 2005, and December 31, 2025, that reported oral manifestations of leprosy were included. Additionally, studies addressing the classification, pathogenesis, clinical features, diagnosis and management, and reactions of leprosy were considered. Review articles, case reports, and short communications were excluded from the study.
A total of 16 articles were selected to evaluate the classification, pathogenesis, clinical features, diagnosis and management, and leprosy reactions. Recent studies reporting the oral manifestations of leprosy were specifically included in the analysis.
Upon entry into the body, Mycobacterium leprae triggers the release of inflammatory cytokines, leading to the activation and proliferation of T- helper (Th) lymphocytes types 1 and 2[1]. These lymphocytes orchestrate the immune response against M. leprae, influencing the clinical manifestations observed in tuberculoid and lepromatous leprosy [5].
In tuberculoid leprosy, a strong cellular immune response limits the proliferation of M. leprae, resulting in fewer bacilli,localized skin lesions,and limited nerve involvement [1,6]. The immune response is predominantly mediatedby CD4+ Th1
cells, which produce high levels of interferon- gamma (IFN-γ), interleukin-2 (IL-2), and tumor necrosis factor-alpha (TNF-α), contributing to effective containment of the infection [7].
In contrast, lepromatous leprosy is associated with a weak cellularimmune response and a predominance of humoral immunity, leading to widespread skin lesions and extensive peripheral nerve involvement [1,6]. This form is characterized by a predominance of CD8+ Th2 cells, which secrete high levels of interleukin-4 (IL-4),interleukin-5 (IL- 5), and interleukin-10 (IL-10),along with low levels of IFN-γ, resulting in poor bacterial control and increased susceptibility to disease progression [8].
Clinical Forms of Leprosy Tuberculoid Leprosy
Tuberculoid leprosy typically presents with annular erythematous plaques, hypopigmented lesions, and elevated borders, which may appear as a singleskin lesion or multiple asymmetric lesions [1,9]. The lesions are generally large, and the lepromin test is usually positive, reflecting a strong cell-mediated immune response against M. leprae [9]. Skin involvement may be associated with alopecia and anhidrosis. Peripheral nerveinvolvement can lead to thickening of the nerve sheathand loss of sensation. Other clinical features may include hypoesthesia, muscle weakness, and facial paralysis when the facial nerve is affected [2].
Lepromatous Leprosy
Lepromatous leprosy presents with numerous, small, symmetrical lesions,including erythematous-brown or hypochromic spotswith indistinct bordersand dry skin [1]. The lepromin test is typically negative, indicating a poor cell-mediated immune response [9]. Lesions commonly affect the face and auricles. Additional features may include preserved sensation, leg edema, formation of lepromas, and leonine facies characterized by facial infiltration and loss of eyelashes[1,10]. Involvement of the earlobes and nasal structures can lead to deformities such as saddle nose.
Indeterminate Leprosy
Indeterminate leprosy is characterized by hypochromic skin patches without loss of sensation or thickening of the peripheral nerves [1,9]. It represents an early, often transient stage of the disease that may progress to more defined clinical forms depending on the host immune response.
Borderline Leprosy
Borderline leprosy is subdivided into borderline tuberculoid, midborderline, and borderline lepromatous forms [1,2].
Borderline Tuberculoid Leprosy: This form resembles tuberculoid leprosy, presenting with large skin lesions, sensory loss, and thickened peripheral nerves [1].
Midborderline Leprosy: Midborderline leprosy is characterized by brown erythematous plaques and foveal spots. Clinically, it displays features of both tuberculoid and lepromatous leprosy. The lepromin test is weakly positive in borderline tuberculoid cases but negative in midborderline and borderline lepromatous forms[9].
Borderline Lepromatous Leprosy: This form resembles lepromatous leprosy, presenting with numerous hypochromic macules and extensive peripheral nerve involvement, reflecting a poor cell- mediated immune response.
Oral Manifestations of Leprosy
Oral and facialinvolvement is most commonly seen in lepromatous leprosy. The prevalence of oral lesions in leprosy patients ranges from 19% to 60%[11]. Oral involvement is often associated with nasal obstruction, leading to mouth breathing, and generally occurs in the late stages of the disease[5]. If left untreated, oral lesions can contribute to facial deformities, significantly affecting patients’ quality of life. Poor oral hygiene in many leprosy patients further increases the risk of dental caries, periodontal
disease, tooth mobility, and other oral health complications.
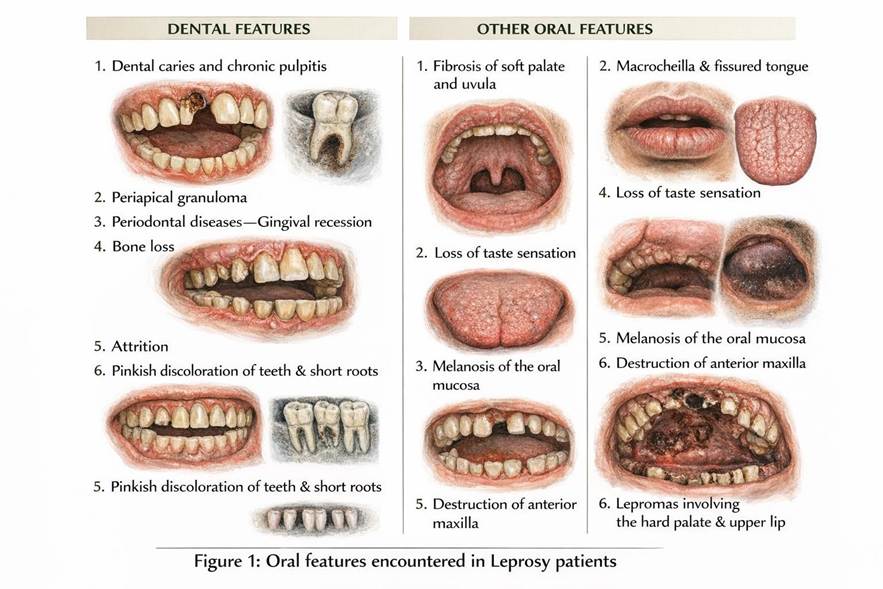
Pallagatti et al. (2012) classified oral lesions in leprosy into leprosy-specific and nonspecific categories.[12] The anterior portion of the hard palate is the most commonly affected site. Specific oral manifestations may include hyperpigmentation of the oral mucosa, macrocheilia, microstomia, lepromas of the lips and palate, nodules on the face, uvula, and buccal mucosa, as well as plaques involving the upper and lower lips [Figure1].
Dental complications associated with leprosy include dentalcaries, anterior maxillarydestruction, periodontal disease, tooth loss, and increased alveolar bone loss, particularly in advanced stagesof the disease [13]. Theseoral and dentalmanifestations underscore the importance of early detection and intervention by dental professionals to prevent functional impairment and improve patient outcomes.
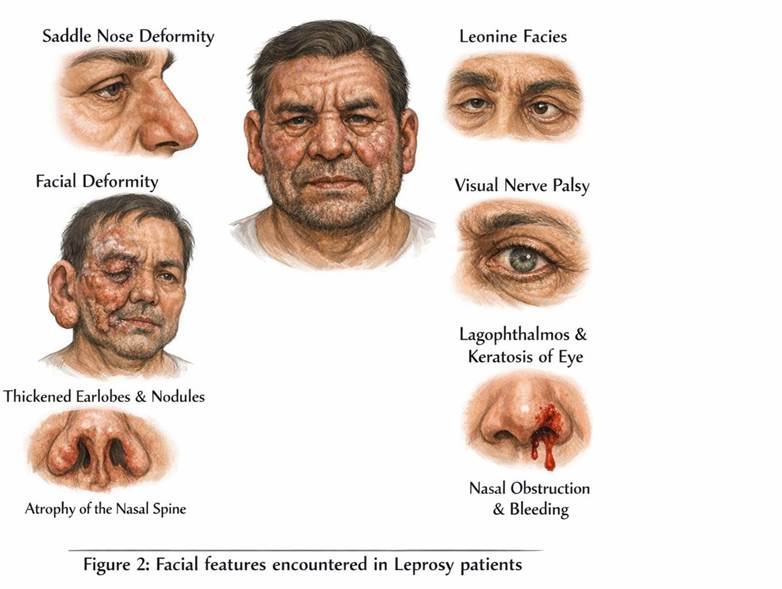
Taheri et al. (2012) reported that leprosy may be associated with facial nerve paralysis, facial deformities, visual impairment, and ocular complications such as lagophthalmos and keratitis.[14] On extraoral examination, patients may present with nodules on the face, thickened earlobes, nodules on the external ear, involvement of nasal structures, nasal obstruction, epistaxis, atrophy of the nasal spine, and loss of eyebrows[15]. [Figure 2]
Pathogenesis of facial and oral manifestations of leprosy
Facial manifestations of leprosy may include sagging earlobes, saddle nose deformity, thinning or loss of eyelashes and eyebrows, and nodular skin eruptions [16]. Mycobacterium leprae shows a predilection for cooler areas of the body,such as the nasal mucosa, which can lead to destruction of the alar and nasal cartilage and ultimately result in saddle nose deformity [17]. Progressive involvement of the anterior face can compromise facial aesthetics and facilitate the spread of infection to the maxillary region.
Sagging of the ears occurs due to infiltration of the earlobes by lepra bacilli, leading to thinning and weakening of cartilaginous tissue. Degenerative changes in ear cartilage may further contribute to ear deformities [16]. Localized infection of the nasal mucosa can extend from the anterior nasal spine to the maxillary incisor region, causing progressive bone loss. This may result in missing maxillary anterior teeth, saddlenose deformity, and loss of the anterior nasal spine, collectively contributing to an unaesthetic facial appearance. Nodules and lepromas of the face are typically observed in the later stages of the disease.
Oral Involvement in Leprosy
M. leprae preferentially infects cooler regionsof the body, including peripheral nerves and the nasal mucosa. Nasal obstruction and stuffiness in leprosy patients often lead to mouth breathing. The most commonly affected oral sites are the hard palate, tongue, buccal mucosa, lips, soft palate, labial and buccal maxillary gingiva, and labial mandibular gingiva. These areas have lower mean temperatures, making them more susceptible to infection; as the mean temperature of an oral site decreases, the likelihood of its involvement increases.
Oral involvement typically begins with the formation of nodules, followed in later stages by fibrosisand functional deformities. Lip involvement
may present as microstomia, macrocheilia, or flat- topped nodules. In advanced disease, the anterior tongue, hard palate, and buccal mucosamay also be affected, leading to tissue infiltration, nodule formation, and scarring. These oral manifestations can compromise both function and aesthetics, emphasizing the importance of early detection and dental care in leprosy patients.
Studies carried out on oral manifestations of leprosy
Castellano et al. (2020) reportedthat the hard palate and upper lip are the most commonly affected oral sites in leprosy, with lesions typically presenting as plaques or lepromas. Their study concludedthat oral lesions are most frequently observed in lepromatous leprosy, borderline lepromatous leprosy, and in patients with erythema nodosum leprosum.[18]
Similarly, Vohra et al. (2019) found that oral manifestations are present in approximately 70% of leprosy patients. Reported lesions included atrophy of the tongue papillae, fissured tongue, chronic generalized periodontitis, loss of taste sensation, melanosis of the oral mucosa, candidiasis, oral submucous fibrosis, aphthous ulcers, depigmentation, and smoker’s palate [19]. These findings highlight the high prevalence and varied presentation of oral involvement in leprosy, emphasizing the importance of early oral examination and dental management.
Raja et al. (2016) reported that leprosy patients frequently exhibit oral conditions such as gingival recession, tooth loss, chronic pulpitis, tooth mobility, dental caries, periodontitis, and dental attrition[20].
Babu et al. (2015) categorized leprosy patients into four groups based on diseaseduration: Group I (0–3 years), Group II (3–10 years), Group III (10–20 years), and Group IV (>20 years).Lepromatous and tuberculoid formswere more prevalent in Groups IV andIII, respectively. Oral manifestations observed included pinkish discoloration of teeth, circumferential enamel hypoplasia, shortened roots, depapillation of the dorsal tongue, fissured tongue, and fibrosis of the soft palate and uvula. These manifestations were more common in patients with lepromatous leprosy compared to tuberculoid leprosy [16].
Pereira et al. (2013) reported poor oral health status among leprosy patients, with high decayed, missing, and filled teeth (DMFT)indices and elevatedplaque levels [15]. Collectively, thesestudies underscore the significant impact of leprosy on oral and dental health and highlight the need for routine dental evaluation in these patients.
Diagnosis and investigations
The diagnosis of leprosy begins with a thorough patient history, including contact with individuals affected by the disease, and clinical evaluation for characteristic signs such as hypochromic skin patches and thickened peripheral nerves. A skin smear can be performed to determine the bacterial load, which is typically high in lepromatous leprosy when examined under light microscopy [21]. The severity of infection correlates with the bacterial index.
Advanced diagnostic methods include polymerase chain reaction (PCR) and serological testing. PCR can detect M. leprae DNA in patients with lepromatous leprosy, whileserological tests identify antibodies specific to M. leprae, aiding in the detection of lepromatous forms[22]. However, these tests are highly specific and cannot reliably confirm all forms of leprosy. For definitive diagnosis and classification, a skin biopsy is recommended, with histopathological findings interpreted in conjunction with clinical features [22].
Histopathology of oral leprosy lesions
Histopathological examination of oral leprosy lesions can reveal a variety of characteristic features. These include the presenceof granulomas, acid-fast bacilli, and perivascular lymphomononuclear and lymphoplasmacytic inflammatory infiltrates [23]. Clinical lesions such as papules,nodules, and ulcers typically demonstrate inflammatory infiltrates along with acid-fast bacilli on histopathology [12,23].
Additional histopathological findings may include epithelial atrophy, dense infiltration of macrophages, absence of the Grenz zone separating the epidermis from the infiltrate, and the presenceof lymphocytes and plasma cells. Hyperkeratosis, vascular congestion, and fibrosis may also be observed, reflecting the chronic and progressive nature of the disease in oral tissues [5,12].
The standard treatment for leprosy is multidrug therapy (MDT),which includes dapsone,rifampicin, and clofazimine [22]. Monotherapy is not recommended due to the risk of developing resistance in M. leprae.
According to the World HealthOrganization (2018), the recommended regimen for multibacillary leprosy consists of 600 mg of rifampicin once per month, 300 mg of clofazimine once per month, and daily doses of clofazimine (50 mg) and dapsone (100 mg) for a period of 12 months.[24] For paucibacillary leprosy, treatment includes 600 mg of rifampicin once per month and a daily dose of 100 mg of dapsone for 6 months[24].
Management of oral manifestations in leprosy patients begins with MDT, accompanied by symptomatic care. Early initiation of treatment is critical to prevent progression to advanced disease and the development of oral lesions. Appropriate antimicrobial therapy may help reduce or prevent oral involvement. Patients should be counseled on maintaining good oral hygiene to minimize disease progression and reduce the risk of secondary dental infections. Dental treatment is recommended to manage caries, periodontitis, and other oral infections, which may otherwise contribute to recurrent or exacerbated leprosy manifestations.
Healthcare providers should follow standard infection control precautions, including the use of gloves, masks, and proper sterilization techniques, to prevent disease transmission. Oral lesions in leprosy are generally reversible with timely and appropriate treatment, but collaboration with a leprologist is essential to ensure comprehensive care and reduce the risk of disease spread.
Reactions of leprosy Leprosy Reactions
Leprosy reactions are immunologically mediated complications that may occur during the course of the disease, often after the initiation of treatment. These reactions are categorized into two types:Type 1 reactions (Reversal Reaction) and Type 2 reactions (Erythema Nodosum Leprosum) [25].
Type 1 Reaction (Reversal Reaction)
Type 1 reactions are characterized by an enhanced cellular immune response, with predominance of CD4+ T cells of the Th1 pattern. This immune activation leads to elevated levels of pro- inflammatory cytokines, including interleukin-1 (IL- 1), interleukin-2 (IL-2), tumor necrosis factor-alpha (TNF-α), and interferon-gamma (IFN-γ) [26]. Type
1 reactions are most commonly observed in borderline forms of leprosy [27].
In patients receiving treatment, Type 1 reactions are associated with a decrease in bacterial load, and the clinical presentation may resemble features of tuberculoid leprosy. Untreated patients may exhibit progressive bacterial proliferation, with clinical features akin to lepromatous leprosy[1].
Clinical manifestations of Type 1 reactions include erythematous plaques on the face and trunk with well-defined borders,hypochromic macules, edema of the face, nasal and labial mucosa, thickened peripheral nerves, neuritis, and associated pain.[28] Prompt recognition and management are essential to prevent permanent nerve damage and disability.
Treatment of Type I reaction
Corticosteroids are the first-line treatmentfor Type
1 leprosy reactions [1]. They reduce edema and suppress the exaggerated cellularimmune response, thereby decreasing inflammation in the skin and peripheral nerves. In borderline leprosy patients, corticosteroid therapy—most commonly with prednisolone—is typically administered for a duration of approximately six months [29].
In cases where corticosteroids alone are insufficient, immunosuppressive agents can be used in combination to improve outcomes. C ommonly employed immunosuppressants include azathioprine and cyclosporine A, which help further modulatethe immune response and control inflammatory damage during Type 1 reactions [30].
Type II reaction
Type 2 reactions predominantly occur in patients with lepromatous leprosy [27]. These reactions are immune-mediated and affect both the skin and systemic organs. The inflammatory responsein ENL is characterized by elevated levels of cytokines, including interleukin-6 (IL-6), interleukin-8 (IL-8), tumor necrosis factor-alpha (TNF-α), transforming growth factor-beta (TGF-β), and interleukin-10 (IL- 10).[15] CD8+ T cells of the Th2 pattern are the predominant immune cells involved in these reactions.
Clinically, ENL presents with symmetrical inflammatory subcutaneous nodules, which may be accompanied by systemic symptoms such as fever, malaise, lymphadenopathy, edema, and arthralgia.[1] Skin lesions may ulcerate or become necrotic. Other organ systems, including the eyes, peripheral nerves, and joints, can also be affected, reflecting the systemic nature of this reaction.
Treatment of Type 2 (Erythema Nodosum Leprosum) Reactions
Mild cases of erythema nodosum leprosum (ENL) are typically managed with non-steroidal anti- inflammatory drugs (NSAIDs) to control inflammation and pain. Moderate-to-severe cases require more intensive therapy, commonly with corticosteroids such as prednisolone, and thalidomide, which has proven efficacy in controlling systemic and cutaneous manifestations [31].
Additional pharmacological optionsthat have shown beneficial effects in ENL include clofazimine, methotrexate, and azathioprine. These agents can be used alone or in combination with corticosteroids or thalidomide to modulate the immune response, control inflammation, and prevent recurrent reactions.