
RESEARCH ARTICLE | DOI: https://doi.org/dx.doi.org/JPHCI/PP.0011
1 Department of Pediatrics, Mahatma Gandhi Medical College and Research Institute, Sri Balaji Vidyapeeth Pondicheery India
2 Department of Pediatrics, Mahatma Gandhi Medical College and Research Institute, Sri Balaji Vidyapeeth Pondicheery India
*Corresponding Author: Kurella Ashwithananda
Citation: Kurella Ashwithananda , (2026) ,Unraveling The Unexplained: The Role Of Genetic Testing In Neonatal Diagnosis And Management – A Literature Review, J. Pediatric Health and Clinical Insights 2(3): dx.doi.org/JPHCI/PP.0011
Copyright  :
© 2026 Kurella Ashwithananda . This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
:
© 2026 Kurella Ashwithananda . This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 16 February 2026 | Accepted: 21 April 2026 | Published: 01 June 2026
Keywords: infant, newborn, genetic testing, chromosomal aberrations, chromosomal microarray analysis,whole exome sequencing,whole genome sequencing, neonatal intensive care units, and congenital abnormalities.
Background
Genetic disorders contribute substantially to neonatal morbidity and mortality, particularly among infants admitted to neonatal intensive care units. Neonatal presentations are frequently nonspecific and include seizures, metabolic instability, hypotonia, dysmorphism, and multisystem involvement, often delaying etiological diagnosis. Advances in cytogenetic and genomic technologies have significantly transformed the diagnostic approach to such neonates.
Methods
A comprehensive literature review was conducted using the PubMed database with Medical Subject Headings related to neonatal genetic testing, chromosomal abnormalities, chromosomal microarray analysis, whole-exome sequencing, whole-genome sequencing, and neonatal intensive care. Studies published between 2010 and 2025 involving neonatal populations were included. Twenty-two key publications were analyzed for diagnostic modalities, diagnostic yield, and impact on clinical management.
Results
Across the reviewed literature, diagnostic yield increased progressively with advancement of genetic technologies. Conventional cytogenetic techniques demonstrated limited diagnostic yield, while chromosomal microarray analysis significantly improved detection of pathogenic copy number variants. Sequencing-based approaches, particularly whole-exome sequencing, consistently showed the highest diagnostic yield, especially in neonates with neurological abnormalities, metabolic disorders, and multisystem disease. Genetic diagnoses frequently influenced therapeutic decisions, prognostication, and genetic counseling.
Conclusion
Genetic testing plays a pivotal role in modern neonatal care by improving diagnostic accuracy and guiding clinical management.
Genetic disorders account for a significant proportion of morbidity and mortality during the neonatal period, particularly among infants requiring admission to neonatal intensive care units 1. It is estimated that nearly one-third of critically ill neonates have an underlying genetic etiology contributing to their clinical presentation2. Neonatal manifestations of genetic disease are often subtle, nonspecific, or overlapping and commonly include seizures, metabolic derangements, hypotonia, respiratory failure, congenital anomalies, or unexplained multisystem involvement. These features frequently complicate early diagnosis and delay targeted intervention.
Historically, the diagnosis of genetic disorders in neonates relied primarily on clinical phenotyping supported by conventional cytogenetic techniques. While these methods enabled detection of major chromosomal abnormalities, they lacked sensitivity for identifying submicroscopic copy number variants and monogenic disorders 3. As a result, many neonates experienced prolonged diagnostic odysseys, repeated investigations, empirical treatments, and uncertainty regarding prognosis and recurrence risk.
Over the past two decades, rapid advances in genomic technology have fundamentally altered the diagnostic landscape of neonatal medicine. Chromosomal microarray analysis enabled genome-wide detection of copy number variants, while next-generation sequencing technologies facilitated comprehensive analysis of monogenic disorders4 5. More recently, rapid and ultra-rapid sequencing workflows have aligned genomic diagnostics with the urgent decision-making timelines of neonatal critical care6 7. These developments have established genetic testing as a cornerstone of precision medicine in neonatology.
This review synthesizes contemporary literature on the role of genetic testing in neonatal care, focusing on the evolution of diagnostic modalities, clinical indications, diagnostic yield, and impact on clinical management.
SEARCH STRATEGY
A structured literature search was conducted using the PubMed database. The search strategy was developed using Medical Subject Headings (MeSH) and relevant keywords including: “Infant, Newborn,” “Genetic Testing,” “Chromosomal Aberrations,” “Chromosomal Microarray Analysis,” “Whole Exome Sequencing,” “Whole Genome Sequencing,” “Neonatal Intensive Care Units,” and “Congenital Abnormalities.”
The search was restricted to human studies, published in English language, between January 2010 and December 2025. The reference lists of eligible studies were also manually screened to identify additional relevant publications.
STUDY SELECTION PROCESS
Identification
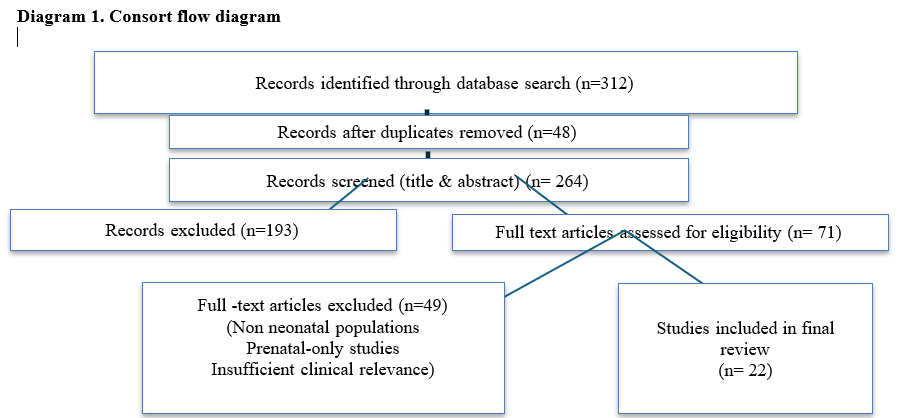
A total of 312 articles were identified through the initial electronic database search across PubMed, Google Scholar, and ScienceDirect.
Screening
After removal of duplicate records, titles and abstracts were screened for relevance to genetic testing in neonates. Following this preliminary screening, 71 articles were shortlisted for full-text review.
Eligibility
The full texts of the shortlisted articles were assessed for eligibility based on predefined inclusion and exclusion criteria.
ELIGIBILITY CRITERIA
Inclusion Criteria
Studies were included if they evaluated genetic testing in neonates based on clinical indications such as dysmorphic features suggestive of an underlying genetic disorder, recurrent or unexplained neonatal seizures, multiple congenital anomalies involving one or more organ systems, or a significant family history including recurrent miscarriages, stillbirths, or unexplained childhood deaths in first- or second-degree relatives. Studies involving inborn neonates admitted to a neonatal unit in whom genetic testing was advised as part of routine clinical care were considered eligible. Articles that reported diagnostic yield, clinical utility, or the impact of genetic testing on clinical decision-making were included. Eligible publications comprised original research articles, observational studies, cohort studies, review articles, and clinical guidelines published in English.
Exclusion Criteria
Studies were excluded if they were conducted exclusively in older pediatric or adult populations without separate neonatal data, were limited to case reports or case series involving fewer than five subjects unless providing significant methodological insight, focused solely on prenatal genetic testing without postnatal neonatal outcomes, lacked adequate methodological detail or clinical relevance to neonatal genetic evaluation, or consisted of non-English publications, editorials, commentaries, or opinion pieces without primary data.
Included Studies
After applying the selection criteria, 22 publications were finalized and included in the qualitative synthesis of this review. The key findings & observations were discussed in the results section. The comprehensive screening process and the application of predefined inclusion and exclusion criteria are illustrated in the CONSORT flow diagram (Diag.1).
LITERATURE REVIEW
EVOLUTION OF GENETIC TESTING IN NEONATAL MEDICINE
During the latter half of the twentieth century, genetic evaluation in neonates relied predominantly on conventional karyotyping, which enabled detection of numerical chromosomal abnormalities and large structural rearrangements such as trisomy’s and monosomies3. Although effective for identifying gross chromosomal anomalies, this approach lacked the resolution required to detect submicroscopic deletions, duplications, and single-gene disorders, which constitute a significant proportion of neonatal genetic disease.
In the early 2000s, targeted molecular cytogenetic techniques such as fluorescence in situ hybridization and multiplex ligation-dependent probe amplification were introduced. These techniques improved diagnostic accuracy for selected microdeletion and duplication syndromes, including Prader–Willi syndrome, Angelman syndrome, and spinal muscular atrophy 8. However, their utility remained limited by the requirement for prior clinical suspicion and restriction to predefined genomic regions.
From approximately 2010 onwards, chromosomal microarray analysis emerged as a transformative diagnostic tool in neonatal medicine. By enabling genome-wide detection of copy number variants at much higher resolution than karyotyping, chromosomal microarray analysis significantly improved diagnostic yield, particularly in neonates with congenital anomalies and dysmorphism4. This led to its recommendation as a first-tier diagnostic investigation in such clinical contexts.
Over the past decade, next-generation sequencing technologies have further revolutionized neonatal genetic diagnostics. Whole-exome sequencing enabled comprehensive analysis of protein-coding regions, allowing identification of monogenic disorders responsible for early-onset neurological, metabolic, immunological, and multisystem disease2 9–13. More recently, whole-genome sequencing and rapid sequencing workflows have expanded diagnostic capabilities while markedly reducing turnaround time, facilitating timely decision-making in critically ill neonates6 7.
INDICATIONS FOR GENETIC EVALUATION IN NEONATES
Genetic testing is increasingly utilized in neonates presenting with clinical features suggestive of an underlying genetic etiology. Evidence from published studies has identified specific neonatal presentations that consistently demonstrate higher diagnostic yields and therefore warrant early genetic evaluation.
Neonates presenting with metabolic abnormalities such as persistent hypoglycemia, metabolic acidosis, hyperammonemia, lactic acidosis, or recurrent metabolic decompensation represent a high-risk group for inborn errors of metabolism. Sequencing-based genetic testing has been shown to enable rapid etiological diagnosis in such cases, allowing early initiation of targeted dietary or pharmacological therapy and prevention of recurrent metabolic crises 9–11.
Neurological abnormalities constitute one of the most frequent indications for genetic testing in neonates. Presentations including neonatal seizures, hypotonia, encephalopathy, movement disorders, and unexplained neurological deterioration have been strongly associated with monogenic etiologies. Multiple studies have demonstrated that whole-exome sequencing yields a molecular diagnosis in approximately forty to fifty percent of neonates presenting with early-onset epilepsy or encephalopathy 12 13. Identification of the genetic etiology has been shown to directly influence antiepileptic drug selection, guide precision therapy, inform prognosis, and assist in long-term neurodevelopmental planning14.
Neonates with multiple congenital anomalies or major structural malformations exhibit a high prevalence of chromosomal abnormalities and copy number variants. Chromosomal microarray analysis has been consistently recommended as a first-tier diagnostic investigation in this group due to its ability to detect submicroscopic deletions and duplications not identifiable by conventional karyotyping4. Diagnostic yields ranging from ten to twenty percent have been reported in such populations15.
Facial dysmorphism, abnormal growth parameters, and disproportionate anthropometric measurements frequently suggest an underlying chromosomal or syndromic diagnosis. Chromosomal microarray analysis is the most employed diagnostic modality in neonates presenting with dysmorphism, as pathogenic copy number variants account for a substantial proportion of these cases16. In selected neonates with persistent clinical suspicion despite nondiagnostic chromosomal microarray analysis, sequencing-based approaches have demonstrated additional diagnostic benefit17.
A positive family history, including recurrent miscarriages, stillbirths, unexplained childhood deaths, or consanguinity, significantly increases the likelihood of genetic etiology. In such contexts, early genetic evaluation facilitates confirmation of diagnosis, accurate recurrence risk counseling, and informed reproductive planning for families18.
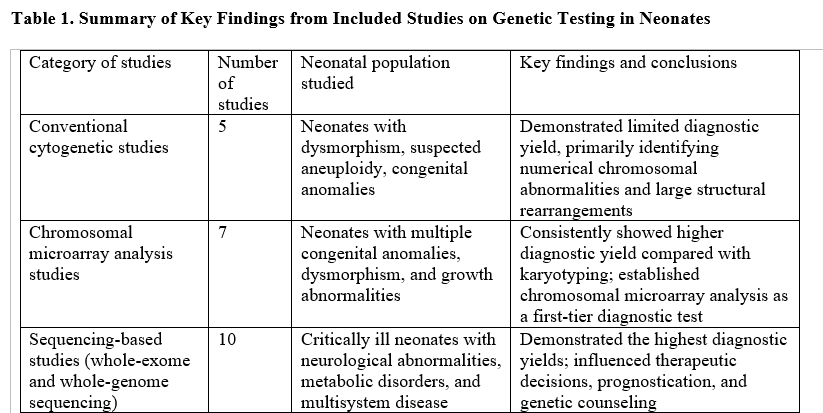
STUDIES INCLUDED AND KEY FINDINGS
The included literature was categorized based on the genetic testing modality evaluated and the neonatal populations studied. Key findings are summarized in Table 1.
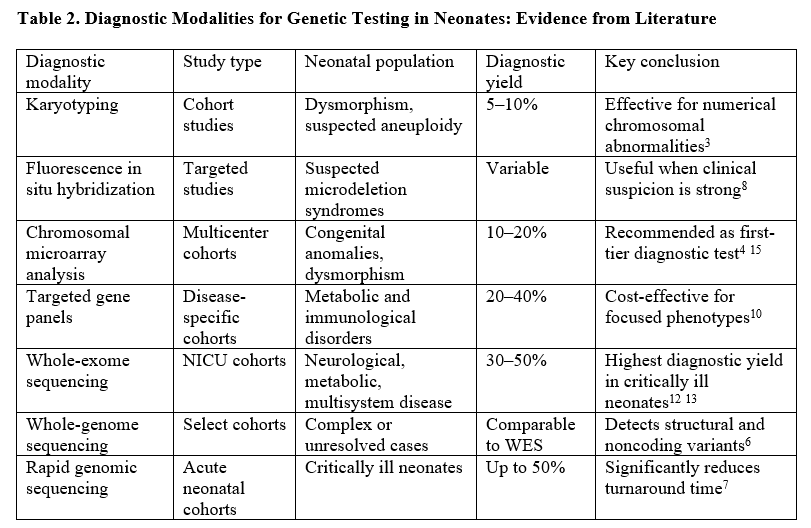
DIAGNOSTIC MODALITIES: EVIDENCE ACROSS LITERATURE
The choice of genetic testing modality in neonates depends on the clinical phenotype, suspected etiology, availability of testing, and urgency of diagnosis. A comparative summary of diagnostic modalities is presented in Table 2.
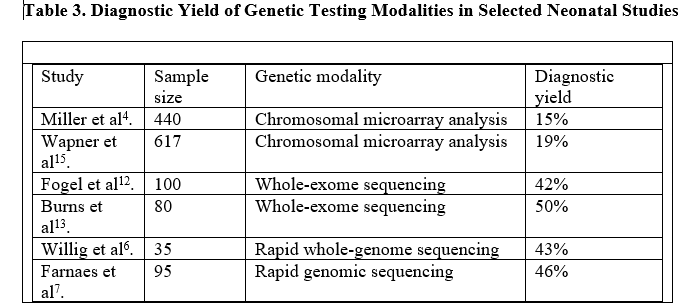
DIAGNOSTIC YIELD ACROSS STUDIES
Across published neonatal cohorts, diagnostic yield has been shown to increase progressively with advancement of genetic testing technologies. Conventional cytogenetic methods identify only a minority of genetic diagnoses, primarily limited to numerical chromosomal abnormalities and large structural rearrangements. Chromosomal microarray analysis significantly improves detection of pathogenic copy number variants, particularly in neonates with congenital anomalies and dysmorphism. Sequencing-based approaches consistently demonstrate the highest diagnostic yields across diverse neonatal presentations, especially in neurological and metabolic phenotypes. Representative diagnostic yields are summarized in Table 3.
CLINICAL UTILITY AND IMPACT ON CLINICAL MANAGEMENT
Genetic testing in neonates extends beyond diagnostic clarification and plays a significant role in guiding clinical management. Identification of a molecular diagnosis frequently enables targeted therapeutic interventions, such as selection of specific antiepileptic medications in genetic epilepsies and initiation of vitamin-responsive or cofactor-based therapies in metabolic disorders1419. Early etiological diagnosis also informs prognostication by allowing clinicians to anticipate disease course, potential complications, and long-term outcomes.
In addition, early genetic diagnosis reduces the need for repeated investigations, invasive procedures, and prolonged empirical therapies by providing etiological clarity. Genetic testing further facilitates family-centered care by supporting accurate counseling regarding recurrence risk, carrier status, and options for prenatal diagnosis in future pregnancies20.
ETHICAL, LOGISTICAL, AND COST CONSIDERATIONS
The expanding application of genetic testing in neonatal medicine raises important ethical, logistical, and economic considerations. Informed consent in the neonatal intensive care setting is particularly challenging, as parents are often required to make decisions regarding complex genomic investigations during periods of emotional distress. Clear communication regarding the scope of testing, potential outcomes, incidental findings, and limitations is essential and requires trained personnel and adequate counseling time19.
Interpretation of variants of uncertain significance remains a major challenge in neonatal genomics. Such findings may not provide immediate diagnostic clarity and can contribute to parental anxiety and uncertainty regarding prognosis. Long-term follow-up, segregation analysis, and periodic reanalysis of genomic data are often necessary to clarify the clinical relevance of these variants, underscoring the need for robust genetic counseling services integrated into neonatal care pathways 20.
Cost remains a significant barrier to widespread implementation of advanced genomic technologies, particularly in low- and middle-income settings. Chromosomal microarray analysis and sequencing-based tests are often expensive and not uniformly accessible. Furthermore, rapid genomic sequencing requires specialized laboratory infrastructure, bioinformatics support, and multidisciplinary expertise, limiting its availability to select tertiary centers21.
EMERGING TECHNOLOGIES AND FUTURE DIRECTIONS
Recent advances in genomic technology continue to reshape neonatal diagnostics. Rapid and ultra-rapid sequencing approaches have demonstrated the feasibility of delivering molecular diagnoses within hours to days, aligning genomic testing with time-sensitive clinical decision-making in critically ill neonates67. These approaches have been associated with shortened diagnostic timelines and earlier initiation of targeted therapy.
Another emerging area is genomic newborn screening, which utilizes sequencing-based technologies to identify actionable genetic conditions not detectable through conventional biochemical screening. Early studies suggest that genomic newborn screening may expand the range of preventable and treatable neonatal disorders; however, ethical concerns related to consent, data storage, result disclosure, and long-term follow-up remain under active discussion22.
The development of population-specific genomic reference databases represents an important future direction, particularly for improving variant interpretation accuracy. Strengthening genetic counseling services and integrating genomic medicine into routine neonatal workflows will be essential for sustainable and equitable implementation.
Published literature consistently demonstrates that chromosomal microarray analysis and sequencing-based technologies offer substantial advantages over conventional cytogenetic methods in neonatal diagnostics. Chromosomal microarray analysis has been widely adopted as a first-tier investigation for neonates with congenital anomalies and dysmorphism due to its superior resolution and diagnostic yield4 15 16. Whole-exome sequencing has emerged as a valuable diagnostic modality across diverse neonatal phenotypes, providing high diagnostic yield in neurological, metabolic, and multisystem disorders12 13. Rapid genomic sequencing further enhances clinical utility by reducing turnaround time and enabling timely therapeutic and prognostic decisions in critically ill neonates67.
Across multiple studies, genetic diagnoses have been shown to influence clinical management, guide targeted therapy, inform prognosis, and support accurate family counseling14 19 20. Despite these advances, barriers related to cost, infrastructure, and interpretation of uncertain findings persist, highlighting the need for continued research, policy development, and capacity building.
Genetic testing has become an integral component of modern neonatal medicine, offering diagnostic clarity, guiding targeted therapy, and supporting informed prognostication and family counseling. Advances in chromosomal microarray analysis and sequencing-based technologies have significantly improved diagnostic yield and transformed neonatal care. Emerging rapid sequencing approaches promise further integration of precision medicine into neonatal practice. Continued investment in genomic infrastructure, ethical frameworks, and genetic counseling services will be essential to ensure equitable and effective implementation of genetic testing for neonates.